Yes, smooth muscle can grow, but not in the way you build biceps at the gym. Smooth muscle, the involuntary muscle lining your airways, blood vessels, uterus, and digestive tract, can enlarge (hypertrophy), multiply in cell number (hyperplasia), and remodel its surrounding tissue in response to sustained mechanical stress, hormonal signals, inflammation, and injury. This is mostly driven by biology and disease processes, not by training or protein shakes. Understanding the difference between these two worlds, the gym kind of muscle growth and the organ-level kind, is what this article is really about.
Can Smooth Muscle Grow? What Causes Thickening and When It Matters

Marcus Kellerman
1 May 2026
What smooth muscle growth actually means in the body
Smooth muscle is fundamentally different from the skeletal muscle you're growing when you lift weights. Skeletal muscle is voluntary, striated, and responds predictably to resistance training through protein synthesis and mechanical tension. Smooth muscle is involuntary, found in the walls of hollow organs and blood vessels, and it doesn't respond to a barbell. When we talk about smooth muscle growth, we're talking about three distinct biological processes: hypertrophy (individual cells getting bigger), hyperplasia (cells multiplying in number), and remodeling (changes in the tissue's composition, thickness, and structural organization). All three can happen, often together, and all three are driven by signals that are largely outside your conscious control.
This is an important distinction because people sometimes wonder whether the muscle-building principles that apply to skeletal muscle, progressive overload, adequate protein, sleep, and so on, also apply to smooth muscle. They largely don't, at least not directly. Smooth muscle operates in a completely different regulatory environment, one governed by hormones, growth factors, mechanical stretch from organ filling or fetal growth, and inflammatory mediators rather than voluntary effort and training load.
Can smooth muscle actually enlarge or multiply? What the evidence says
The short answer is yes, definitively. Research in asthma physiology is probably the clearest window into this. In asthmatic airways, smooth muscle mass increases through both hypertrophy and hyperplasia, meaning cells get bigger and there are more of them. Bronchial biopsies from patients with mild-to-moderate asthma show measurably increased smooth muscle cell numbers compared to healthy controls, and the broader body of evidence points to coordinated increases in both cell size and cell count in more severe disease.
Interestingly, some individual studies find that hyperplasia (more cells) rather than hypertrophy (bigger cells) is the dominant mechanism, which highlights how the balance between these two processes can shift depending on the organ, the severity of the condition, and how the measurement is done.
Vascular smooth muscle tells a similar but more nuanced story. These cells are remarkably adaptable. They can switch between a contractile phenotype, which is the normal state focused on regulating blood vessel tone, and a synthetic phenotype, which is oriented toward proliferation and extracellular matrix production. This phenotype switching is central to how vascular smooth muscle grows and remodels in disease states. In conditions like atherosclerosis and intimal hyperplasia (the thickening of artery walls after injury), smooth muscle cells proliferate, migrate, and lay down collagen and other matrix proteins, leading to measurable wall thickening. So yes, smooth muscle can grow. But the mechanisms and triggers are organ-specific and largely tied to pathology or major physiological events like pregnancy.
Real conditions that cause smooth muscle to thicken
Here are the most well-documented examples of smooth muscle growth happening in real human bodies, organized by organ system.
Airways: asthma and COPD

Airway remodeling in asthma is one of the most studied examples of pathological smooth muscle growth. The changes include increased airway wall thickness, increased smooth muscle mass from both hypertrophy and hyperplasia, and altered tissue composition. This isn't just a functional change, it's structurally measurable in biopsies. The increased smooth muscle mass contributes to the narrowing and stiffening of the airways, which is why asthma management focuses on controlling the inflammation and signals that drive this remodeling, not just on reversing bronchoconstriction in the moment.
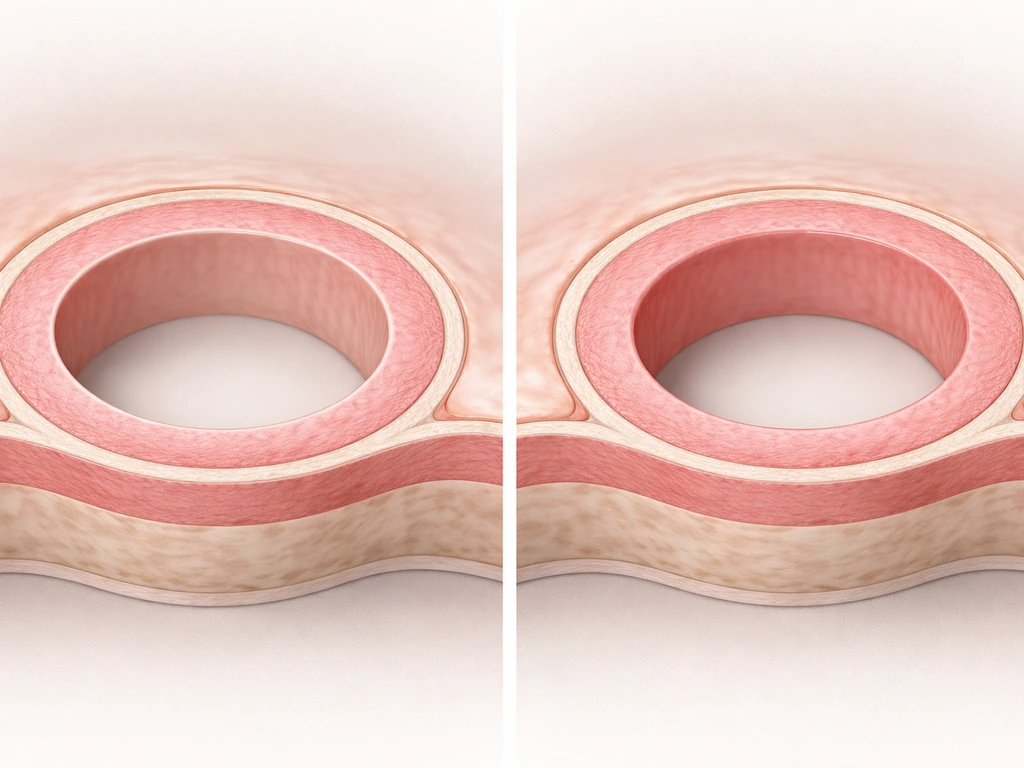
Blood vessels: hypertension and atherosclerosis
Chronically elevated blood pressure forces vascular smooth muscle to work harder against sustained mechanical load. Over time, this leads to vascular remodeling, with smooth muscle cells shifting phenotype, proliferating, and producing extracellular matrix that thickens the artery wall. In atherosclerosis, smooth muscle cells migrate into the intima (the inner layer of the vessel), proliferate, and create a fibrous cap over plaques. The vascular smooth muscle that gets more of these cells is not stronger in any useful sense, it's part of a disease process that narrows the vessel and raises cardiovascular risk.
Uterus: pregnancy

The uterus is one of the most dramatic examples of smooth muscle growth in normal human physiology. The myometrium (the uterine smooth muscle layer) grows substantially during pregnancy to accommodate a growing fetus. Early pregnancy growth appears to be driven primarily by hyperplasia, new smooth muscle cells forming, while later gestation growth shifts to hypertrophy, with individual cells enlarging, alongside remodeling of the extracellular matrix.
Research specifically supports that mechanical stretch from fetal growth drives the hypertrophic response in the third trimester. Research in the myometrium during pregnancy supports that mechanical stretch drives the hypertrophic response [mechanical stretch from fetal growth drives the hypertrophic response](https://pubmed. ncbi. nlm.
nih. gov/19776098/). The uterus then largely returns to its previous state after delivery, making pregnancy a remarkable example of reversible smooth muscle growth.
Gastrointestinal tract
The GI tract's smooth muscle can also adapt structurally to chronic changes in mechanical load. Conditions involving chronic obstruction or altered motility can lead to hypertrophy of the smooth muscle layers in the gut wall as the tissue responds to sustained resistance or stretching. This is less frequently highlighted in fitness conversations, but it follows the same basic logic: sustained mechanical or chemical stress on smooth muscle tissue can trigger remodeling over time.
What signals actually drive smooth muscle to grow
Smooth muscle growth is controlled by a very different set of signals than skeletal muscle hypertrophy. Where skeletal muscle growth is triggered primarily by mechanical tension and anabolic hormones like testosterone and IGF-1, smooth muscle responds to a broader and more organ-specific signal environment.
- Mechanical stretch: Sustained stretching of smooth muscle, from a growing fetus in the uterus, elevated intraluminal pressure in blood vessels, or chronic obstruction in the gut, activates mechanosensitive pathways that drive hypertrophy and remodeling. This is the closest analog to 'overload' that smooth muscle experiences.
- Growth factors: Platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-beta), and epidermal growth factor (EGF) all play documented roles in smooth muscle cell proliferation and phenotype switching. TGF-beta, in particular, is tied to the fibrotic and synthetic phenotype changes seen in vascular disease.
- Hormones: Estrogen and progesterone are major regulators of uterine smooth muscle growth during pregnancy. In vascular smooth muscle, angiotensin II, a hormone central to blood pressure regulation, is a well-known driver of proliferation and hypertrophy.
- Inflammation: Inflammatory mediators like interleukins and leukotrienes are strongly implicated in airway smooth muscle remodeling in asthma. Chronic low-grade inflammation acts as a persistent growth signal for smooth muscle in multiple organ systems.
- Phenotype switching: Vascular smooth muscle cells can shift from a contractile phenotype to a synthetic phenotype, downregulating structural proteins like smooth muscle myosin heavy chain (MYH11) and alpha-smooth muscle actin (ACTA2) while upregulating matrix proteins like collagen (COL1A1, COL3A1) and vimentin. This switch enables proliferation and matrix production.
None of these signals are something you control through a workout or a supplement protocol. They're driven by your body's physiological state, pathological conditions, or major biological events like pregnancy. This is what makes smooth muscle so different from skeletal muscle when we're talking about intentional growth.
Can exercise or supplements meaningfully increase smooth muscle mass?
This is the question most people in a fitness context are really asking, and the honest answer is: not in any direct, meaningful, or controllable way. Exercise does produce systemic effects that reach smooth muscle, but the adaptations are not the same as skeletal muscle hypertrophy and they're not something you can target or measure on a scale or in a mirror.
Regular aerobic exercise, for example, promotes favorable vascular remodeling, including improved endothelial function and reduced arterial stiffness, but this is not the same as growing vascular smooth muscle. In fact, exercise generally reduces the pathological drivers of vascular smooth muscle thickening by lowering blood pressure and inflammation over time. So if anything, consistent cardio training is likely to reduce pathological smooth muscle growth in blood vessels rather than increase smooth muscle mass.
Resistance training doesn't have a meaningful direct effect on smooth muscle tissue. The hypertrophy response from lifting is almost entirely confined to skeletal muscle. Protein intake, creatine, branched-chain amino acids, and the rest of the conventional muscle-building supplement stack all work through pathways that are specific to skeletal muscle protein synthesis. They don't meaningfully stimulate smooth muscle hypertrophy or hyperplasia in healthy people.
If you've come across content suggesting you can 'train' your smooth muscle like you train your glutes or your back, that content is misleading. The organs that contain smooth muscle are not accessible to intentional progressive overload in the gym sense. The closest thing to a controllable lever would be something like consistently eating large meals, which does produce stretch on GI smooth muscle, but this is not a practical or desirable muscle-building strategy.
For readers interested in related questions, such as whether specific facial muscles respond to targeted training, or whether the masseter muscle can grow through chewing, those questions involve skeletal or mixed muscle tissue and follow different rules than what's described here.
When smooth muscle growth is actually a problem
This is where the conversation shifts from interesting physiology to something genuinely important for your health. In most of the contexts described above, smooth muscle growth is either a sign of disease or a complication of one. Treating it like a fitness goal would be a mistake.
| Organ/Context | Type of Growth | Why It's a Problem |
|---|---|---|
| Airways (asthma/COPD) | Hypertrophy + hyperplasia of airway smooth muscle | Permanently narrows airways, worsens obstruction, reduces treatment response |
| Blood vessels (hypertension) | Vascular smooth muscle thickening, phenotype switching | Stiffens arteries, raises cardiovascular disease risk |
| Arteries (atherosclerosis/intimal hyperplasia) | SMC proliferation, fibrous cap formation, ECM deposition | Narrows vessel lumen, raises heart attack and stroke risk |
| Uterus (fibroids) | Smooth muscle tumor (leiomyoma) | Can cause heavy bleeding, pain, and fertility problems |
| GI tract (obstruction-related) | Hypertrophy of gut wall smooth muscle | Indicates underlying obstruction; worsens motility issues |
Uterine fibroids deserve a specific mention because they are extremely common. Fibroids are benign tumors made largely of smooth muscle tissue (leiomyomas). They're driven by estrogen and progesterone, and they represent a form of smooth muscle growth that is directly relevant to a huge proportion of people with a uterus. They are not caused by exercise or diet, and they cannot be resolved by changing your training program.
The broader red flag here is this: if you're experiencing symptoms that might be related to smooth muscle in a specific organ, whether that's breathing difficulty, unexpectedly high blood pressure, unusual GI symptoms, or reproductive system changes, the cause is not a fitness variable. It's a medical variable, and it requires medical evaluation.
Practical next steps: how to approach this the right way
If you landed here because you're genuinely curious about muscle biology, the takeaway is clear: smooth muscle can and does grow, through hypertrophy, hyperplasia, and remodeling, but it's driven by biological conditions you can't replicate with a workout or supplement protocol. Your fitness focus should stay on skeletal muscle, which is the muscle that actually responds to training, nutrition, and recovery. If you want the practical answer to how to grow smooth muscle, the key is knowing which organ and condition you mean, because the triggers are not the same as gym training.
If you landed here because you have symptoms, that's a different conversation. Here's what actually makes sense to do.
- See a doctor for organ-specific symptoms. Breathing difficulties, high blood pressure, GI motility problems, or reproductive symptoms all need a clinical evaluation. Blood pressure can be checked in minutes. Airway function can be assessed with spirometry. Uterine issues require imaging.
- Don't try to self-treat smooth muscle conditions with fitness strategies. No supplement stack, training program, or dietary approach has demonstrated meaningful clinical benefit for pathological smooth muscle remodeling. Some may help with systemic inflammation reduction, which has indirect benefits, but they're not treatments.
- If you have asthma or COPD, talk to your doctor specifically about airway remodeling and whether your current management plan is addressing it. Inhaled corticosteroids and other controllers work in part by reducing the inflammatory signals that drive smooth muscle growth.
- If you have hypertension, treat it consistently. Managing blood pressure is one of the most direct ways to reduce the mechanical stress driving vascular smooth muscle thickening. Exercise, sodium reduction, and medication (if indicated) all play real roles here.
- If fibroids or other uterine smooth muscle issues are suspected, get an ultrasound. Treatment options range from watchful waiting to hormonal therapy to surgical approaches depending on symptoms and severity.
- If you're interested in the related science of skeletal muscle growth in specific areas, like facial or jaw muscle development, those questions have their own evidence base and practical guidance that's more directly actionable from a fitness standpoint.
The bottom line is that smooth muscle growth is real, well-documented, and biologically significant. Can the masseter muscle grow? The same idea applies: smooth muscle does not adapt like skeletal muscle, and the jaw's muscle has different biological drivers. If you're wondering how to grow masseter muscle, the jaw is still a different biological driver than what this article describes for smooth muscle. But it's not something you build in the gym. It's something your body manages in the background, usually for good physiological reasons, and sometimes in ways that signal a problem worth addressing with medical support rather than a training plan.
FAQ
If smooth muscle can grow, does that mean I can “train” it by doing more cardio, lifting, or taking supplements?
Not in a targeted, measurable way. The smooth-muscle changes that are best documented are organ- and condition-specific (asthma remodeling, vascular disease, pregnancy). Regular exercise can reduce harmful drivers like high blood pressure and inflammation, which generally lowers the risk of pathological thickening rather than producing intentional smooth muscle hypertrophy.
What’s the difference between smooth muscle thickening and “more muscle” in general?
Smooth muscle growth can involve bigger cells (hypertrophy), more cells (hyperplasia), and changes in surrounding extracellular matrix (remodeling). In diseases like atherosclerosis or intimal hyperplasia, wall thickening often reflects matrix and tissue organization changes, not improved “strength” of the vessel.
Does smooth muscle growth always mean disease?
No. Pregnancy myometrial growth is a normal example that is largely reversible after delivery. Outside of major physiological states like pregnancy, many prominent cases are linked to pathology (asthma, atherosclerosis, post-injury vessel thickening, fibroids).
Why do people sometimes claim you can increase smooth muscle size with specific exercises or “stretching”?
Because stretching can change mechanical load and symptoms short-term, but it does not create the same regulatory signals as the organ-level processes that drive hypertrophy or hyperplasia. For GI smooth muscle, for example, chronic obstruction or altered motility can drive remodeling, but intentionally trying to stretch or overeat is not a safe or reliable “training” strategy.
Can smooth muscle hyperplasia happen in humans, or is it mostly theoretical?
Hyperplasia has been observed in human airway disease. In asthma research, increased smooth muscle cell number in biopsies supports both enlargement and increased cell count. In other organs, the dominant contribution can vary, but the idea is not just theoretical.
Is vascular smooth muscle growth the same as getting “bigger” arteries from exercise?
Exercise-induced vascular benefits are different. Improvements in endothelial function and reduced arterial stiffness are generally protective and do not equal a pathological increase in smooth muscle mass. Persistent hypertension and vascular injury are the classic conditions associated with maladaptive smooth muscle proliferation and matrix buildup.
Can uterine fibroids be reduced by changing workouts or diet?
Fibroids are driven by reproductive hormones and represent a form of smooth-muscle tumor growth. Exercise and diet may help overall health, but they do not reliably eliminate fibroids or their underlying growth drivers.
If I’m trying to understand my symptoms, how do I know whether smooth muscle involvement is likely?
Look for organ-specific patterns: breathing symptoms with known asthma-like triggers (airway remodeling), persistent elevated blood pressure (vascular changes), chronic constipation or obstruction-type symptoms (GI motility and possible smooth muscle hypertrophy), or heavy/prolonged bleeding and pelvic pressure (possible uterine smooth muscle fibroids). New, worsening, or unexplained symptoms should prompt medical evaluation rather than self-treatment as a fitness issue.
What are common mistakes people make when reading about smooth muscle growth?
Treating it like a gym target, assuming protein shakes or creatine would drive smooth muscle cell growth, or trying to “measure” adaptation at home (there is no practical mirror-and-scale equivalent). Another mistake is ignoring red-flag symptoms and delaying evaluation for possible underlying disease.
What should be my next step if I suspect an organ condition involving smooth muscle?
Start with a medical assessment tailored to the organ system involved. That may include lung evaluation for asthma-related symptoms, blood pressure and cardiovascular risk assessment for vascular concerns, GI evaluation for persistent motility or obstruction symptoms, or gynecologic evaluation for fibroid-related symptoms. The key point is that the workup identifies the trigger, because the fix is not training-based.


